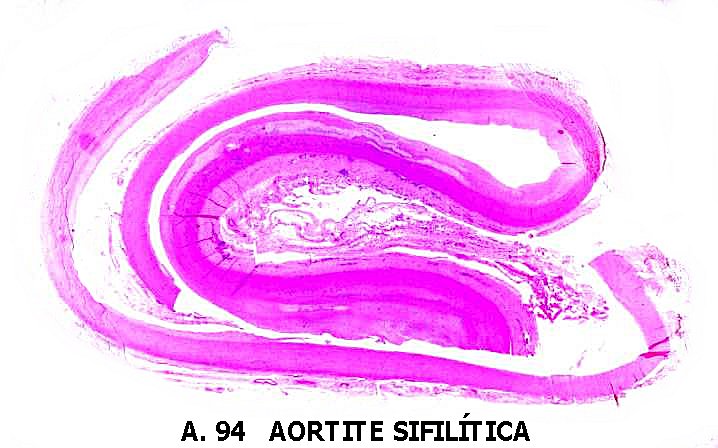
Syphilitic aortitis is the principal cardiovascular manifestation of syphilis. Syphilis does not ordinarily affect the cardiac valves, although the aortic valve commissures may be separated. Rarely, it may affect the myocardium. It may affect the coronary arteries more often, but usually only the proximal few centimeters of these vessels are involved. Syphilitic aortitis may be complicated by aortic insufficiency, angina pectoris, and aortic aneurysm. Syphilitic aortitis is usually recognized 10 to 30 years after the initial primary chancre, but occasionally only a few years after the original infection. The disease produces aortic medial destruction with necrosis of smooth muscle and elastic tissue and periarterial inflammation with lymphocyte cuffing of the vasa vasorum.
There is also mtimal wrinkling with treebark formation and a tendency to narrow the orifice of the coronary arteries and to dilate the aortic root. Innominate artery aneurysm may occur, but more distal arterial aneurysms are unusual. The syphilitic process, unlike arteriosclerosis, is usually more intense in the aortic mot than in the distal aorta. Congenital syphilis seldom produces aortitis. Because of the delay in clinical manifestations, patients with syphilitic aortitis are ordinarily more than 30 years of age when recognized clinically and are usually over 50 years of age when syphilitic aneurysms are recognized. Uncomplicated syphilitic aortitis ordinarily produces no symptoms and may be recognized only at the autopsy table. It produces dilation and perhaps calcification in the ascending aorta. The latter may be detected radiologically.
SYPHILITIC AORTIC ANEURYSM.
Aneurysms occur in 10 to 40per cent of patients* with syphilitic aortitis. Syphilitic aneurysms, once the most common cause of thoracic aneurysms, are much less common than a few decades ago. Nearly half occur in the ascending aorta, 30 to 40 per cent in the arch, and 15 per cent in the descending thoracic aorta. Syphilitic aortic aneurysms may occur in the abdominal aorta but are distinctly uncommon there, especially if there is no syphilitic aneurysm in the thoracic aorta. With ascending aortic aneurysm, aortic insufficiency is often present; rarely, there is a visible pulsatile mass in the first and second right intercostal spaces with exaggerated pulsations of the right sternoclavicular |otnt or in the epistemal notch.
Chest pain, the most common symptom, may occur owing to rib, sternal, or vertebral erosion. The pain is usually substernal, in the dorsal spine, or at the side of the chest. Increasing intensity of pain is usually an ominous sign associated with impending rupture. A chest radiogram may demonstrate erosion of ribs and sternum by the aneurysm. Respiratory difficulty may indicate that the aneurysm is in the arch of the aorta; there may be a tracheal tug; hoarseness and a brassy cough suggest recurrent laryngeal nerve paralysis There may be Homer’s syndrome with ptosis, miosis, and decreased sweating on the left side of the face.
There may be decreased sweating on the left side of the face. There may be superior vena caval obstruction with distended nonpulsahle jugular veins, dyspnea, and collateral venous circulation over the thorax. Today, however, more than 95 per cent of supenor caval obstruction is caused by malignant tumors. Aortic arch aneurysm may produce compression of the left mainstem bronchus, with atelectasis of the left lung or of the left lower lobe. Hemoptysis suggests tracheal or bronchial ulceration Hematemesis may indicate rupture into the esophagus In the descending thoracic aorta, rarely the aneurysm mav present as a pulsatile mass medial to, or inferior to, the angle of the left scapula. In these cases, vertebral erosion may occur. Cardiac enlargement does not occur because of aneurysm alone.
Radiologic studies are helpful in diagnosing thoracic aneurysm of any cause. Calcification limited to the ascending aorta suggests syphilitic aortitis but may occur with other vaneties of aortitis, healed dissection, and arteriosclerosis. A mass continuous with the aorta with calcification in its wall is very likely an aneurysm. Without calcification aortic aneurysm must be distinguished from other mediastinal masses, especially tumors of lymph nodes, dermoid cysts, thymic tumor, and substemal thyroid gland. Evaluation of pulsations of a mass by fluoroscopy is virtually worthless; pulsatory movements transmitted into contiguous tumors are indistinguishable from those of intrinsic pulsations of the aorta. Conversely, aneurysms which are lined with thrombus may fail to show visible pulsations. Contrast aortography is the precise way of settling the diagnosis. CT scans with intravenous contrast medium enhancement will often obviate the need for contrast aortography.
Course and Prognosis of Syphilitic Aortitis.
Syphilitic aneurysms tend to rupture eventually. The rupture may take place into the right or left pleural space, into the trachea or esophagus, or into the pulmonary artery, where it produces a continuous murmur like that of patent ductus arteriosus. The aneurysm may rupture into the right heart, producing a continuous murmur like that described under Congenital Aortic Aneurysm, above. Laplace’s law states that tension in walls of a cylinder is equal to the product of pressure times radius. Hence the tension in the wall of an aortic aneurysm is greater than that in the adjacent aorta. Surgical resection of syphilitic aneurysms is recommended when feasible and when the patient does not suffer from some other disease which materially limits life expectancy.
Antisyphilitic Treatment of Syphilitic Aortitis
The Venereal Disease Control Advisory Committee recommended that patients who have cardiovascular syphilis receive benzathine penicillin, 2.4 million units intramuscularly weekly for three successive weeks, or aqueous procaine penicillin, 600,000 units intramuscularly daily for 15 days. Such therapy may not allay the progression of syphilitic aortitis or aneurysm, as the weakened aortic wall continues to expand despite the absence of active infection.
Conclusion
Syphilitic aortitis is a serious condition that should not be overlooked. Early detection, prompt treatment, and preventive measures are essential in managing this silent attacker. If you experience any concerning symptoms or have a history of syphilis, it is crucial to consult a healthcare professional for proper evaluation and management. By prioritizing your cardiovascular health, you can take proactive steps towards a brighter and healthier future.