Cardiac amyloidosis is a disease of unknown cause characterized by the widespread tissue deposition of an amorphous hyaline-like substance. The disease is uncommon under age 40 and affects the sexes equally. The prevalence of amyloidosis in the general population is not known. Although patients with multiple myeloma may have an incidence of amyloidosis as high as 15 per cent, it occurs in less than 1 per cent of unselected cases at autopsy. The relationship of amyloidosis to the aging process is of particular interest, as it has been found in as many as 90 per cent of patients dying of senile dementia when specifically looked for in brain, heart, or pancreas.
Amyloidosis presents clinically most often with renal involvement, especially the nephrotic syndrome, congestive heart failure, carpal tunnel syndrome, sprue, penpheral neuropathy, or orthostatic hypotension. The most common symptoms are fatigue, weight loss, edema, dyspnea, and, to a lesser extent, hoarseness, paresthesias, or the carpal tunnel syndrome. Although the edema may be produced by either the nephrotic syndrome or congestive heart failure, the presence of dizziness, syncope, and orthostatic hypotension should suggest cardiac amyloidosis.
On physical examination hepatomegaly, splenomegaly, and macroglossia are usually found, the last being more common in patients with multiple myeloma. In addition, there may be lymphadenopathy, especially in the submandibular region, purpura, and skin lesions. The cardiac manifestations may simulate constrictive pericarditis because of impaired ventricular filling during diastole and include an elevated jugular venous pressure with a rapid “y” descent and an early diastolic filling sound. However, if the left heart is more severely involved, the signs of left heart failure may predominate.
The electrocardiogram shows low voltage, which may falsely suggest constrictive pericarditis, as well as Q wave abnormalities, which may be misinterpreted as old myocardial infarction. Supraventricular arrhythmias are frequently seen, as well as the entire spectrum of conduction abnormalities. Patients with cardiac amyloidosis are particularly susceptible to digitalis-induced arrhythmias, possibly because of the infiltration of amyloid in the perivascular region of the sinoatrial node.
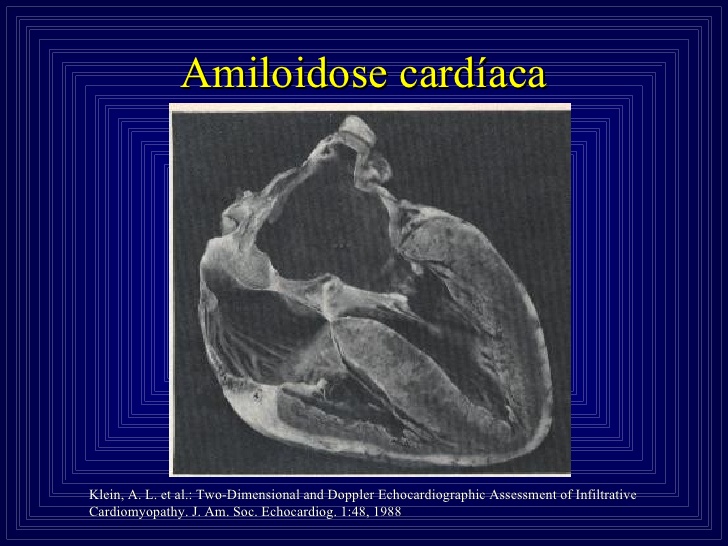
Pathologically, the heart is increased in size and firm in consistency. Nodular lesions may be seen in the endocardium, valves, and pericardium. Histologic examination reveals diffuse interstitial infiltration of amyloid within the myocardium and in the blood vessels. Amyloid is identified by its distinctive green birefringence when stained with Congo red and examined under a polarizing microscope.
Pathologically, the heart is increased in size and firm in consistency. Nodular lesions may be seen in the endocardium, valves, and pericardium. Histologic examination reveals diffuse interstitial infiltration of amyloid within the myocardium and in the blood vessels. Amyloid is identified by its distinctive peen birefringence when stained with Congo red and examined under a polarizing microscope.
The clinical diagnosis is proved by tissue biopsy from the rectum in over 80 per cent of patients, and in more than 90 per cent when tissue is obtained from the kidney, carpal tunnel, or liver, making it essentially unnecessary to resort to endomyocardial biopsy. Two-year survival for patients with primary amyloidosis is 35 per cent, but only 10 per cent for those with amyloidosis associated with multiple myeloma. Congestive heart failure is the most common cause of death, and sudden death, presumably from arrhythmias, also frequent.