The rhinoplasty , also known as nose reshaping surgery , is one of the most requested cosmetic surgery. Rhinoplasty allows you to change the shape and size of the nose, improving the harmony of the face without distorting its physiognomy.
More precisely, cosmetic nose surgery allows you to increase or decrease the size of the nose (too small, too large or too wide), change the shape of the back (hollow or with the presence of a hump or hump) and of the tip (too large, too narrow or too long), change the width of the nostrils and change the angle between the forehead and nose or between the nose and upper lip. This surgery can be performed in all forms of the nose although the most frequent are the typology of the Caucasian, Asian and African race.
With this type of intervention, whose history dates back to 2000 BC. C. , it is also possible to correct post-traumatic or present defects from birth and respiratory problems. If breathing difficulties are caused by the deviation of the nasal septum it is necessary to proceed simultaneously with a “septoplasty” intervention in order to model and reposition the deviated nasal septum.
PRIMARY, SECONDARY AND ETHNIC RHINOPLASTY
Based on the history of the intervention, the patient’s ethnicity and the technique used, rhinoplasty is called primary or secondary, ethnic, closed or open. Rhinoplasty is defined as primary when it is performed for the first time to correct congenital or acquired blemishes. Secondary rhinoplasty, on the other hand, aims to eliminate those defects that could not be corrected with the first surgery or that were caused by previous rhinoplasty. Sometimes some patients need further interventions (tertiary, quaternary rhinoplasty, etc.) due to the importance of the trauma suffered or the severity of the malformation from which they are affected (cleft lip and palate, etc.). Ethnic rhinoplasty is aimed only at patients of Asian or African-American origin who wish to obtain a modification (so-called “westernization”) of their features. The ethnic rhinoplasty it is a particularly complex cosmetic surgery as the patients of Asian and African-American origin have skin, subcutaneous, conformation and consistency characteristics of the osteo-cartilaginous structures different from those of the patients of Caucasian origin.
CLOSED AND OPEN RHINOPLASTY (OPEN RHINOPLASTY AND CLOSED RHINOPLASTY)
Depending on the technique used by the surgeon, we speak of “closed” or “open” rhinoplasty .
The closed rhinoplasty is indicated for noses which have small defects, especially at the tip, or which do not show large deviations of the nasal pyramid. With this technique it is possible to correct very well the nose defects which however must not have big asymmetries. In closed rhinoplasty all incisions are made inside the nose. The surgeon operates using a front light and all changes to the nasal pyramid are performed by passing through the nostrils. This technique is particularly difficult and is used only by very experienced surgeons.
The open rhinoplasty is used to correct major defects of the tip as asymmetries, bulbous tip, nose “pinocchio”, “pinched-nose” tip bifida, diverted, retracted, etc., Or to correct outcome of cleft lip and palate, or in secondary rhinoplasty or post-traumatic. This technique provides, in addition to the incisions made in “closed” rhinoplasty, also an incision on the columella (ie at the base of the nasal pyramid). Even this technique, if correctly performed, does not leave visible scars. “Open” rhinoplasty is easier to perform because it allows the surgeon to directly see the defects of the osteo-cartilaginous structures to be corrected.
If the patient has an excessive width of the nostrils, a further surgical method can be associated with the closed or open rhinoplasty which allows to reduce the size and shape of the nostrils by means of longitudinal or transverse incisions made at the base of the nose. Since there is no single technique valid for all types of surgery, a good surgeon should know and be able to perform both techniques depending on the defect that is to be corrected. Furthermore, rhinoplasty can be performed alone or in association with functional nose surgery (rhinoseptoplasty, nasal polyps and turbinate surgery).
ARE THERE ANY AGE LIMITS FOR SUBJECT TO RHINOPLASTICS?
There are no age limits to undergo this type of intervention, but it is preferable to wait for the end of the development of bone and cartilage structures which generally takes place around 15-16 years. In particular, in young women it is possible to perform a rhinoplasty from the age of 15, while in men it is necessary to wait for 16 years, as the maturation of the structures in the male sex arrives with about 12 months later than the female one.
WHAT OTHER INTERVENTIONS CAN BE CARRIED OUT TOGETHER WITH RHINOPLASTICS?
Rhinoplasty can be performed alone or in combination with other surgical techniques such as blepharoplasty, facelift, mentoplasty or other cosmetic or functional surgery ( septoplasty ).
WHAT ARE THE RISKS AND COMPLICATIONS OF THIS TYPE OF INTERVENTION?
The of nose reshaping surgeryit is one of the most difficult and complex cosmetic surgery. When this type of surgery is performed by a specialist in plastic surgery, experienced in modeling the nose and in authorized structures, the results are generally very good. However, it is a real surgical procedure where complications (bleeding, infection) are rare but can happen and be easily overcome only if the intervention is performed by a specialist in plastic surgery within duly authorized structures. To reduce the risk of complications, however, it is essential to follow exactly the advice and instructions that the surgeon will give you before and after the operation. Smokers should decrease the
HOW IS THE PRE-OPERATIVE VISIT DONE?
Rhinoplasty is a very personalized intervention which, as such, requires an accurate specialist visit. During the first visit, the surgeon will have to evaluate the shape and size of the nose, check for any aesthetic and / or functional defects and show you the possible harmonic modifications of the shape, profile and aesthetics of your nose. These corrections can be viewed through the computerized processing of digital photos of your face. The surgeon will also need to assess your health to rule out complications (such as high blood pressure, clotting or scarring problems) that could affect the final outcome of the surgery. At the end of the visit, the surgeon, in agreement with you, will choose the shape of the nose that best suits the physiognomy and aesthetics of your face. Before the operation you will receive specific instructions on pre and post-operative nutrition and on the intake of drugs, alcohol and cigarettes.
WHAT TYPE OF ANESTHESIA IS PRACTICED?
Rhinoplasty is generally performed under general anesthesia with hospitalization in day surgery queens. Only in more complex cases may hospitalization for one or two nights be necessary. Sometimes modest rhinoplasty can be performed under local anesthesia with sedation (this means that you will be awake but relaxed and insensitive to pain).
ARE THE ENGRAVINGS VISIBLE?
The incisions are absolutely invisible as they are hidden inside the nasal cavities.
and falling tip.
HOW LONG DOES THE INTERVENTION LAST?
The rhinoplasty operation lasts about an hour, is completely painless and ends with the application of a small plaster stopped on the back of the nose with two patches, but without the use of tampons.
WHAT IS THE POST-OPERATIVE COURSE FOR A RHINOPLASTIC INTERVENTION?
In the 48 hours following the rhinoplasty operation you will have to rest with your head raised. Starting from the third day you can resume a normal life but avoiding strenuous activities, saunas and Turkish baths, exposure to the sun, taking very hot food and drinks and limiting the use of glasses as much as possible. Swelling and bruising around the eyes may appear in the first two days. Very rarely bleeding that requires the use of tampons can occur. Seven days after the operation, the surgeon will proceed with the removal of the plaster and your nose, initially swollen and edematous, will assume day after day the harmonic form that had been agreed before the intervention.
WHAT TYPE OF RESULT CAN BE OBTAINED?
Rhinoplasty allows to obtain very satisfactory results for both the patient and the plastic surgeon. The result, generally very good and appreciable already after the first two weeks, will be definitively achieved about one year after the intervention.
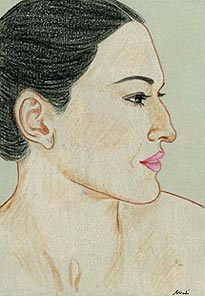
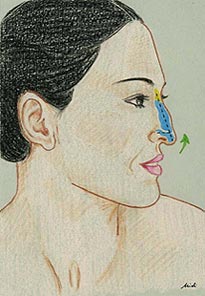
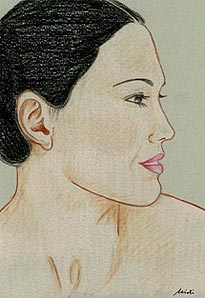
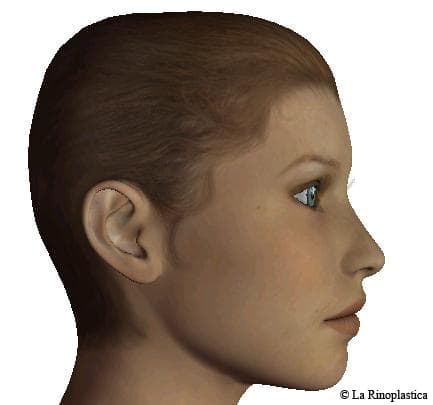
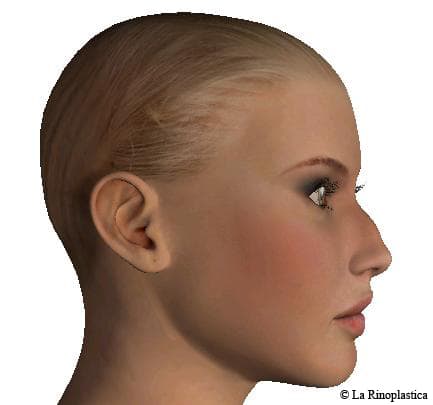
Case 1
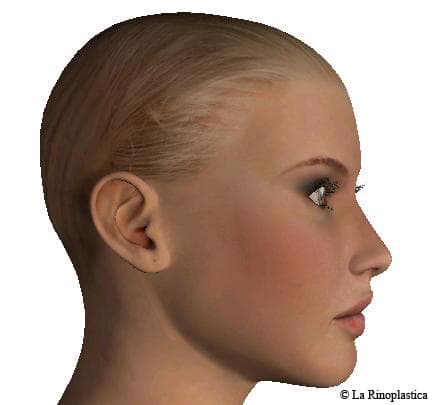
Case 2
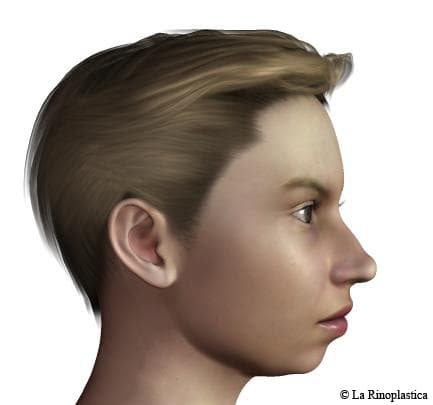
Case 3
Case 4






profiloplasty
The term “prophyloplasty” is used to indicate a series of cosmetic surgery operations aimed at obtaining a complete remodeling of the profile of the face through the correction of the nose, chin and / or cheekbones. The cosmetic surgery operations used in prophylasty are rhinoplasty , mentoplasty and malaroplasty . These interventions can be performed simultaneously or at different operating times. During the specialist examination, it is possible to simulate on the computer the corrections of the facial profile that the surgeon deems most appropriate.
RHINOPLASTY: COSTS
The rhinoplasty has a price very variable. A simple rhinoplasty can cost from € 6,500 to € 8,500 .
A rhinoseptoplasty has a cost of around € 8,500 .
A secondary tertiary or quaternary rhinoplasty can have a cost that can range from € 8000 to € 12,000 .
RHINOPLASTIC FAQ
Q. In rhinoplasty who decides the shape of the nose? The patient or the plastic surgeon?
A. The choice of the shape and size of the nose is generally made by the plastic surgeon in agreement with the patient, trying to respect as much as possible the physiognomy of the face and the physical characteristics of the patient. For example, if the patient is very tall, it is not recommended to have a French nose, i.e. with the tip very raised as most people, being of short or medium height, would end up seeing only the nostrils. In a man, then, it is preferable to have a straight nose even if a little more important than a small, upturned nose. Sometimes the surgeon may suggest to make even slight changes to the chin or cheekbones to make the face more harmonious and proportionate.
Q. Can rhinoplasty also solve breathing problems?
A. Yes. Septoplasty can be associated with rhinoplasty surgery when necessary in order to correct deviation of the septum or other respiratory problems.
Q. After how long will I be able to resume my sport activity?
A. After a rhinoplasty operation, it is advisable not to expose yourself to the risk of trauma for at least a month, which is the time required for the ossification process of the nose to be perfected.
D. I would like to have nose surgery but I don’t know which surgeon to turn to. How do you choose a good plastic surgeon?
A. Nose remodeling surgery is one of the most difficult and complex cosmetic surgery. When this type of surgery is performed by a specialist in plastic surgery, experienced in modeling the nose and in authorized structures, the results are generally very good. What matters in the choice of the plastic surgeon is the experience, seriousness, skill and aesthetic sense of the surgeon. To this end, it may be useful to inquire about the number of operations performed by that professional, to see photos of the operated patients (before and after the intervention), and to examine together the possible harmonic modifications of the shape, profile and aesthetics of your nose. . These corrections can be viewed through the computerized processing of digital photos of your face,
Q. I would like to know if swabs are always needed in rhinoplasty and if they are painful.
A. Personally, when I perform a rhinoplasty I do not use internal swabs (which can cause a lot of pain when they are removed), even when I have to carry out a septoplasty together with rhinoplasty. Only rarely (in about 2% of cases) may it be necessary to apply swabs to cope with unexpected bleeding.
Q. Is rhinoplasty painful? What kind of anesthesia is practiced?
A. Rhinoplasty is not a painful operation. Some patients report that they felt pain during the surgery or when they removed the tampons. In reality, the operation is not absolutely painful because it is performed either under general anesthesia (i.e. the patient is completely asleep) or under local anesthesia with sedation (this means that the patient is awake but relaxed and insensitive to pain). I also prefer not to use swabs unless this is made necessary to cope with unexpected and excessive bleeding.
Q. In what structure can a rhinoplasty be performed?
A. Rhinoplasty is generally performed under general anesthesia with hospitalization for one or two nights. Sometimes modest rhinoplasty can be performed under local anesthesia with sedation (this means that you will be awake but relaxed and insensitive to pain) and in a day-hospital regime.
Q. After a rhinoplasty, can the nose be reopened and for how many times?
A. After a rhinoplasty operation, adjustments can be made, even if subsequent operations are increasingly difficult to perform and aesthetic improvements less and less guaranteed, especially when it comes to reconstructing a nose that has become excessively small following the first surgery or excavated.
Q. After how many days can I be seen in public?
R. The answer is very subjective. Some people have no problem going out with the patches and plaster on the nose (which will be removed after 7 days from the surgery), while others prefer to wait for the swelling and hematoma that often appear immediately after the surgery and that may persist for about 7-10 days, they completely reabsorbed. However, most patients are already presentable immediately after the removal of the plaster.
Q. When can I put my glasses back on?
A. The use of glasses is not recommended for at least a month. If it is not possible to use contact lenses, it will be necessary to hold the glasses with the hand, avoiding that the frame rests on the nose.
Q. After the removal of the plaster will my nose have assumed the final shape or will it still have to settle down?
R. After the removal of the plaster the nose will appear much more swollen and edematous than the harmonic form that had been agreed before the intervention, especially on the tip of the nose. The final aesthetic result, appreciable already after the first two weeks, will be definitively achieved about a year after the intervention.
D. I’d like to have a nose piercing. It’s safe? If I have to change my mind later, will the hole close on its own or will the sign remain?
A. Being a foreign body, the piercing can be a vehicle for small bacterial infections that could damage the subcutaneous tissues and cartilages of the nose. Once done, there will always be a small sign that can eventually be corrected under local anesthesia but which will still leave an inevitable scar on the nose.
Q. How do you apply for funding for rhinoplasty surgery?
R. It is possible to request the payment in installments of the rhinoplasty intervention, asking your cosmetic surgeon what are the methods of financing cosmetic surgery in cases where there is no immediate financial availability to pay for an intervention.
D. Anatomically, how is the nose made?
R. The nasal pyramid, which constitutes the external part of the nose, is formed by a scaffolding partly bony and partly cartilaginous. The bony part consists mainly of the two bones of the nose, which are joined at the top with the nasal process of the frontal bone, and laterally with the ascending portion of the maxillary bones. The cartilage part is made up not only of the quadrangular cartilage, which forms the nasal septum, of the triangular cartilages (also called lateral cartilages) and of the tip cartilages (also called cartilages of the nasal or wing wings). There are also small cartilaginous formations called sesamoids, of variable number and size, placed in the spaces left free by the major cartilages. The tip cartilages, one on each side, they are corolla-shaped and concur to form the nostrils (lateral crus) and the support column of the nasal pyramid (crus mediale) called columella. The muscles of the nose act on the wings of the nose, narrowing and widening the nostrils: the triangular and myrtle-shaped muscles are constricting muscles, while the lifting muscles of the wing of the nose and of the upper lip have a dilating function. The nasal cavities, or nasal pits, appear as long channels separated from each other by an osteo-cartilaginous wall, called the nasal septum. They communicate anteriorly with the outside by means of the nostrils and posteriorly with the nasopharynx, by means of the coane. The nasal septum is constituted, posteriorly, by a bony part and, anteriorly, by a cartilaginous part. The bony part is formed by the perpendicular lamina of the ethmoid and the ploughshare, from the maxillary bone and palatine. The cartilaginous part that joins the free margins of the aforementioned bony laminae completes the septum forward and consists of a lamina which, due to its shape, takes the name of quadrangular cartilage of the septum, and from the medial crus of the winged cartilage called columella. The lateral wall of the nasal passages is one of the most important parts for breathing; in it, in fact, the turbinates and the meatus are found: in the latter the paranasal sinuses, the ethmoidal cells and the nasolacrimal canal blossom. The turbinates are raised formations, stretched from front to back, arranged in overlapping planes and are made up of mucous and bone tissue. They have the function of humidifying the air that enters the nasal pits before it arrives in the nasopharynx. The turbinates are four on each side and are named (from bottom to top): lower turbinate, medium turbinate, upper turbinate and supreme turbinate (not always present). In the space below each turbinate there is a meatus that takes its name from the turbinate above it (lower, middle and upper meatus). The nose has a respiratory and olfactory function. As regards the respiratory function, the inhaled air, once entered the nasal cavities, follows a precise route: after being influenced by the shape and orientation of the nostrils, the air passes through the pre-turbinal region, touches the head of the inferior turbinate moves towards the middle meatus, passes below the middle turbinate and exits through the choruses. This air flow breaks against the lower and middle turbinate and forms vortices of which one follows the lower meatus and another goes back to the olfactory region. The latter current is of great importance for the olfactory perception. In the expiratory phase, the air follows the same path as the inspiratory one, passing mainly along the lower meatus. As regards the olfactory function, the sensory cells of the sense of smell are bipolar neurons specialized in the reception of odors and are placed in the upper part of the nasal septum, above the superior or supreme turbinate. The human being can distinguish between 2,000 and 4,000 smells. the air follows the same path as the inspiratory one, passing mainly along the lower meatus. As regards the olfactory function, the sensory cells of the sense of smell are bipolar neurons specialized in the reception of odors and are placed in the upper part of the nasal septum, above the superior or supreme turbinate. The human being can distinguish between 2,000 and 4,000 smells. the air follows the same path as the inspiratory one, passing mainly along the lower meatus. As regards the olfactory function, the sensory cells of the sense of smell are bipolar neurons specialized in the reception of odors and are placed in the upper part of the nasal septum, above the superior or supreme turbinate. The human being can distinguish between 2,000 and 4,000 smells.