Sandfly fever is a viral disease characterized by fever, headache, ocular pain, conjunctiva injection, and malaise followed by complete recovery. it is also called Pappataci Fever It occurs during the hot, dry season in parts of the European and African littoral of the Mediterranean, Asia Minor, the Russian shores of the Black Sea, Pakistan, and northwest and central India, where the vector fly, Phlebotomus papatasi, exists.
Etiology.
The disease is caused by two small (about 25 m/x) antigenically unrelated viruses (Sicilian and Neapolitan) with closely similar properties, including a common, restricted host range (man, newborn mice, or, after adaptation, intracerebrally inoculated weaned mice). Both types can be propagated with cytopathic effect in several cell cultures, primary mouse (best) or human kidney and He-La. Complement-fixing and hemagglutinating antigens can be prepared from brain tissue of infected newborn mice. Strains of both types, adapted to adult mice by Sabin, produce immunizing infections in man with no disease (Sicilian type) or negligible disease (Neapolitan type). Several viruses newly isolated from Brazil, Panama, Iran, and Pakistan, including some from febrile patients, are antigenically related to the Neapolitan type, which, thus, becomes the prototype of a new arbovirus group.
Epidemiology Sandfly fever .
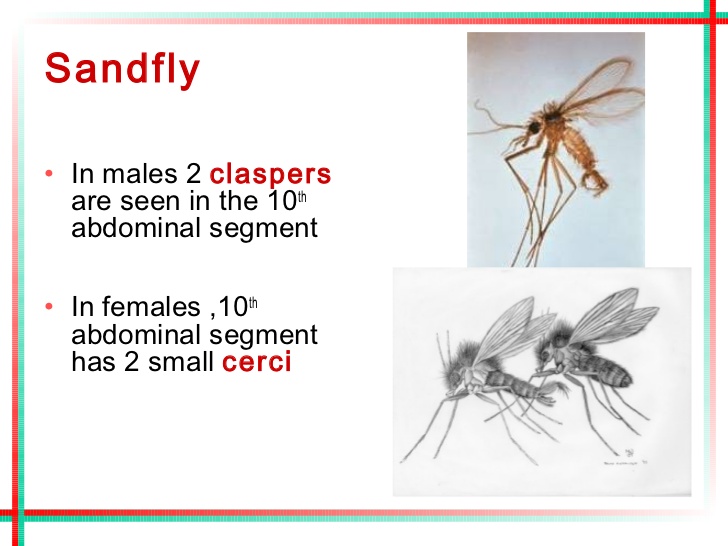
The only known mechanism for virus maintenance is the man-vector (Phlebotomus papatasii female) cycle. The vector has a flight range of up to 200 yards, tends to stay close to ground level, and, because of its small size, readily penetrates conventional screens and mosquito netting. It thrives best in hot, dry periods, breeding in organic debris beneath stones and in cracks in masonry or other equivalent sites.
Its life span is short, perhaps no more than two to three weeks. Recovery of Neapolitan group viruses from females of the phlebotomus subgenus, Ser- gentomyia, suggests a possible new vector.The basic reservoir mechanism remains undetermined. Viral persistence in the hot, dry season is adequately explained by serial transmissionsbetween susceptible humans via the vector. Recovery of a virus from phlebotomus males (Barnett and Suyemoto> supports the earlier disputed observation of transovarial transmission as a possible mechanism of virus overwintering.
Geographic distribution and seasonal occurrence are determined by the distribution and activity of the vector. In endemic areas, the majority of the inhabitants presumably experience unrecognized immunizing infections in infancy or early childhood and disease is virtually restricted to newcomers. Large outbreaks require substantial immigration, such as troop movements.
Pathogenesis and Pathology.
Because fatalities do not occur, the pathologic processes are unknown. However, extensive experimental infection of man during World War II (Sabin, Philip, and Paul) has provided much data on pathogenesis. Regular induction of disease requires use of the intracutaneous or intravenous rather than the subcutaneous or intramuscular paths for infection. The usual incubation period is three to six days. Viremia begins 24 hours before onset and endures only about two days. Postinfection immunity to homologous challenge lasts at least two, years and is evidenced, by low-level antibody response that is best shown by the neutralization test. There appears to be no postinfection immunity to heterologous challenge.
Clinical Manifestations of Sandfly Fever .
The experimental infections of man permitted close scrutiny of etio- logically certain disease. Inapparent infections were rare. Onset typically is sudden, with fever reaching its peak (not more than 104.5° F.) in 24 to 48 hours and subsiding usually in two to four days. In relation to the temperature, the pulse is disproportionately rapid early in the illness but slow later. Other common signs and symptoms are frontal headache, photophobia, ocular * pain, severe conjunctival injection, erythema of the face and neck (but no true rash), aches or pains in the back and extremities, stiffness in the neck, various gastrointestinal manifestations including constipation early and diarrhea later, sore -throat, and chilliness. Moderate leukopenia is usual. The cerebrospinal fluid is unchanged. In about 5 per cent of patients, fever and symptoms recur after five to seven days of convalescence.
Diagnosis and Treatment.
The differential diagnosis includes malaria, prevaricate viral hepatitis, influenza, and dengue. Recognition of the disease is usually based on clinical and epidemiological grounds, i.e., outbreaks of brief febrile illness in the hot, dry season among tourists or other immigrant groups. Although recovery of blood- borne virus in suckling mice and detection of neutralizing antibody response are possible, exclusion of other viral infections is the usual role of the viral laboratory. Only symptomatic treatment is available.
Prognosis of Pappataci Fever.
In addition to occasional recurrence of febrile disease, as already noted, convalescence is characterized by weakness and sweating and occasionally, by severe but transitory mental depression. Full recovery is apparently invariable.
Prevention
No vaccine of established value is generally available. Effective vector control is feasible, using residual DDT or other insecticidal sprays for dwellings and nearby breeding sites, supplemented by repellents such as dim-ethyl- naphthalene to guard against possible attack after sundown.
Sandfly Fever, also known as Phlebotomus fever or three-day fever, is a viral illness transmitted by the bite of infected sandflies. The illness is caused by a group of viruses belonging to the genus Phlebovirus. I’ll create a tabular guide to explain how Sandfly Fever works, covering aspects like transmission, symptoms, treatment, and prevention.
Sandfly Fever: A Tabular Guide
| Aspect | Description |
|---|---|
| Cause | Caused by viruses of the Phlebovirus genus, transmitted by sandfly bites. |
| Transmission | Transmitted through the bite of infected female sandflies, primarily during the warmer months. |
| Symptoms | – Fever (lasting 3-5 days) <br> – Headache <br> – Muscle and joint pains <br> – Eye pain <br> – Anorexia <br> – Nausea |
| Diagnosis | – Blood tests to detect the virus or antibodies. <br> – PCR (polymerase chain reaction) tests. |
| Treatment | – No specific antiviral treatment. <br> – Symptomatic relief (e.g., pain relievers, fever reducers). |
| Prevention | – Avoiding sandfly bites (using insect repellents, bed nets, protective clothing). <br> – Environmental control measures to reduce sandfly populations. |
| Complications | Rare; can include meningitis or encephalitis in severe cases. |
| Incubation Period | Usually 3-7 days after the bite of an infected sandfly. |
| Endemic Regions | Common in the Mediterranean, Middle East, parts of Asia, and Africa. |
This table provides a concise overview of the key aspects of Sandfly Fever. It’s important to note that while the disease can be uncomfortable, it is generally self-limiting and most people recover without any specific treatment. However, prevention, especially in endemic areas, is crucial.