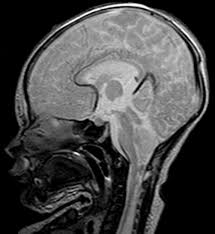
Arnold-Chiari Malformation is characterized by downward displacement of the cerebellum through the foramen magnum of the skull and by similar caudal elongation of the medulla. These cases can be divided into two major types, the infantile and the adult.
Infantile Form.
The infantile form is commonly associated with other mid-line defects such as spina bifida and meningocele, hydrocephalus due to aqueductal or fourth ventricular obstruction, and other congenital malformations of the brain and cord. The infantile form of the Amold-Chiari malformation usually presents itself because of hydrocephalus in the early months of life, with evidence of spina bifida or frank paraparesis due to myelomeningocele. Therapy is directed toward surgical relief of the hydrocephalus with a ventricular shunting procedure and repair of the meningomyelocele. Prognosis is poor for patients with extensive defects.
Adult Form OF Arnold-Chiari malformation.
The malformation may be asymptomatic until adult life, when there is the onset of symptoms and signs of damage to the cerebellum, lower cranial nerves, pyramidal tracts, and posterior columns. The presenting signs may be due to hydrocephalus secondary to obstruction of the cerebrospinal fluid pathways or to coexisting syringomyelia of the cervical spinal cord and medulla (see Hydrocephalus and Spinal Cord Tumors). Commonly, there is evidence, clinical orroentgenographic, of fusion of the cervical vertebrae, platybasia, or basilar impression. The Arnold-Chiari malformation in adults may simulate syndromes produced by tumors near the foramen magnum and by multiple sclerosis. Surgical enlargement of the foramen magnum and decompression of the cervicomedullary junction are beneficial in selected cases.