Although the types of meningitis caused by various infective agents share much in common, the differences dictate that they be considered separately.
ACUTE BACTERIAL MENINGITIS
The brains of patients dying during the early days of meningitis are frequently swollen, and temporal lobe or cerebellar herniations are found in more than 25 per cent of cases. The purulent subarachnoid exudate may be several millimeters in thickness or barely visible. It accumulates in sulci, along major veins and venous sinuses, in basal cisterns about the cerebellum, and over the dorsal aspect of the spinal cord. The ventricular walls are lined or flecked with pus in about half the cases. There is polymorphonuclear infiltration of small arteries and veins in about a third and thrombosis of vessels (usually veins) in 10 per cent of cases. An occluded venous sinus is found rarely. Infarction (frequently hemorrhagic of cerebral tissue is a common consequence of thrombosis of vessels. Necrosis of cerebral cortex in the absence of demonstrated vascular occlusions is also seen, particularly beneath major accumulations of exudate.
In such areas there is a diffuse polymorphonuclear infiltration of the tissue: imaged neurons, increased numbers of activated microglia (histiocytes) and astrocytes are also found. The pathogenesis of these cortical changes is uncertain, but toxic bacterial effects have been postulated. Similar changes are seen in the ventricular walls, often denuded of ependymal cells. A granular ependymitis may result from an abundant proliferation of subependymal astrocytes and, together with fibrosis of the leptomeninges, it may persist as the major residual finding in meningitis; hydrocephalus is a well, recognized complication of such changes. It should be noted that a postmortem examination performed many weeks to years after recovery from meningitis often reveals no residual abnormalities.
Clinical Neurologic Manifestations. Acute Stage.
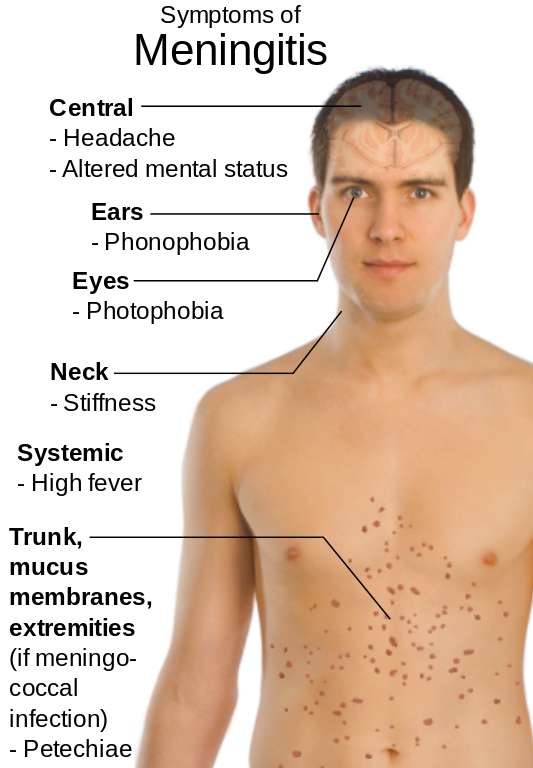
The symptoms and signs of meningitis may develop explosively de novo or may appear in the waning stages of an infection localized elsewhere e.g., respiratory tract. Headache, backache, nausea, and vomiting are common symptoms, and nuchal rigidity occurs in more than 80 per cent of cases. Kernig and Brudzinski signs are frequently present. Only in the neonate and very young infant is meningitis often unattended by evidence of increased pressure and meningeal irritation. Even fever may be absent at this age. Photophobia may be a prominent early symptom and is related in some way to the meningeal inflammation (it occurs also in subarachnoid hemorrhage).
Disturbances in mental status occur in nearly every case of acute bacterial meningitis. Irritability, confusion, delirium, and stupor are common; coma occurs in about 10 per cent of cases and indicates a poor prognosis. Focal or generalized seizures occur in about a fourth of all patients with meningitis, being encountered much more frequently in infants, who have a greater susceptibility to seizures. Signs
of cerebral dysfunction, other than altered consciousness and seizures, are infrequent in acute bacterial meningitis and appear most often when treatment has been delayed. They include disturbed conjugate gaze, dysphagia, paresis of extremities, and visual field defects. When transitory they may represent postictal phenomena. Striking and persisting signs are usually due to bacterial encephalopathy or to infarction of tissue due to cortical venous thrombosis (see Cortical Thrombophlebitis).
The latter complication commonly develops during the second week of disease when signs of infection and meningeal irritation are subsiding. Bilateral neurologic signs and convulsions occurring first on one side and then on the other always suggest an associated thrombosis of the superior sagittal sinus. Prominent and slowly progressive focal signs appearing early in the course of meningitis should bring to mind the pos. ibility of an associated focus of sepsis such as subdural empyema, brain abscess, or bacterial endocarditis with cerebral embolism.
Perhaps 5 to 20 per cent of patients develop cranial nerve palsies during the acute stage of bacterial meningitis. Impaired ocular movement, deafness, and labyrinthine dysfunction are most frequently seen, but blindness and facial paralysis also occur. Most cranial nerve palsies are probably attributable to the meningeal exudate, but the eighth nerve complex may be damaged by bacteria or their toxins acting directly on the inner ear. Despite the fact that the cerebrospinal fluid pressure is usually elevated, papilledema is rare and more characteristic of brain abscess, subdural empyema, or venous-sinus thrombosis.
Being A Doctor,You Must Know Causes And Types of Meningitis
The infrequent occurrence of papilledema in uncomplicated meningitis is probably explained by the short duration of increased pressure. Nevertheless, the heightened intracranial pressure, when present, is a disturbing finding, for death may result from the syndrome of transtentorial or foramen magnum herniation. Administration of excessive amounts of hypotonic fluids during treatment of meningitis should be avoided, for water intoxication may further elevate the intracranial pressure.
Collections of xanthochromic fluid containing a high concentration of protein (200 to more than 1000 mg. per 100 ml.) and, at times, inflammatory cells and bacteria may be recovered from the subdural space in up to 50 per cent of infants during the course of acute bacterial meningitis, but this complication is not recognized in adults.
Late Neurologic Sequelae.
Neurologic sequelae are found in about 5 per cent of adults and 20per cent of infants and children surviving an attack of acute -bacterial meningitis. One of the more serious complications of meningitis is hydrocephalus, which develops in about 2 per cent of patients (usually infants). This is most often attributable to fibrosis of the- meninges and consequent obliteration of the major basilar cisterns. Less often a noncommunicating hydrocephalus results from obliteration of the foramina of Magendie and Luschka, and rarely from ependymitis and narrowing of the aqueduct. Aside from monocular blindness and permanent deafness, which complicate meningitis in 3 to 5 per cent of cases, enduring dysfunction of cranial nerves is unusual. Residual parenchymatous damage following meningitis causes epilepsy in 4 per cent, impaired mental functions or retardation in 3 per cent, and hemiplegia or bilateral hemiplegia in 2 per cent of patients.
NONSUPPURATIVE MENINGITIS
Tuberculous Meningitis. Initial involvement of the central nervous system in tuberculosis usually occurs during a period of transient hematogenous dissemination. Tubercles of macroscopic or microscopic size can be demonstrated in the meninges in virtually every case of tuberculous meningitis. Tuberculomas of the central nervous system and of the meninges do not necessarily lead to frank meningitis, however. This subject is discussed in the articles on Tuberculous ‘Meningitis and Tuberculomas.
Mycotic Meningitis. Fungi, although ubiquitous in nature, cause human disease infrequently and rarely involve the nervous system. Impairment of host defenses, as in leukemia, lymphomas, diabetes, and with immunosuppressive treatment, often predisposes to the development of mycotic infections. The possible coexistence of two disease processes, therefore, demands consideration whenever the physician is confronted by a patient with meningitis due to a fungus. A chronic granulomatous meningitis with mononuclear inflammatory cells and giant cells of the Langhans type is produced by most of the fungi pathogenic to man; torulosis, caused by Cryptococcus neoformans, is the most frequently encountered type of mycotic meningitis. The illness may be protracted, relapsing, and remitting over many years; less often it is subacute or acute.
The reactive fibrosis of the meninges in infections due. to Aspergillus fumigatus may be extreme, and occasionally may produce symptoms of a meningeal mass lesion. Involvement of small meningeal vessels, at times producing a necrotizing angiitis, is a feature of Histoplasma capsulatum meningitis but this rarely leads to hemorrhage from or thrombosis of the vessel. By contrast, in mucormycosis large veins and arteries are frequently occluded by extension of the infection into their walls and lumina.
The infection commonly arises in the ancillary air sinuses in patients with diabetes mellitus and extends in a retrograde manner’ to involve the sagittal sinus and carotid artery. A diffuse encephalitis, solitary granuloma, or true cerebral abscess may also develop in the course of a mycotic infection in man. The symptoms and signs of brain tumor may be simulated by a mycotic abscess. Although treatment of intracranial fungal infections with amphotericin B has brightened the therapeutic possibilities considerably, the mortality rate remains high.
Sarcoidosis
Involvement of the nervous system occurs in about 3 per cent of cases of Boeck’s sarcoid, but sarcoidosis is a rare cause of aseptic meningitis. The granulomatous lesions of this disease tend to accumulate about blood vessels, particularly at the base of the brain. Infiltration of the optic chiasm and hypothalamus can result in amblyopia and diabetes insipidus. Hydrocephalus and increased intracranial pressure may develop. Diagnosis depends upon ancillary clinical data or upon a histologically typical lesion obtained from tissue biopsy (see article on Sarcoidosis). The mortality rate is high when symptoms and signs of intracranial disease develop.
Neoplastic Meningitis
Diffuse infiltration of the leptomeninges by primary intracranial or metastatic malignant tumors may produce symptoms and signs of meningitis. The cerebrospinal fluid findings can include pleocytosis, elevated protein, and greatly reduced glucose concentrations. Recognition of neoplastic cells in the fluid will permit accurate diagnosis.
Viral Meningitis
A table listing the viral agents that may produce meningitis is included in the discussion of Viral Meningitis in the section on Microbial Diseases. Aseptic meningitis caused by Leptospira is easily confused with that caused by viral agents, and must be considered in any differential diagnosis. In viral meningitis variable numbers of mononuclear cells are found in the leptomeninges and about blood vessels in Virchow- Robin spaces. The process usually excites minimal reactions of meningeal fibroblasts.
Typically, the induced illness is acute, mild, of “brief duration, and is followed by complete recovery. Fever, malaise, headache, vomiting, and meningeal symptoms and signs can be expected, and seizures may occur in young children. When consciousness is significantly impaired or there are other prominent focal or generalized signs of involvement of the central nervous system, the term viral meningitis is inappropriate, and the designation meningoencephalitis or encephalitis should be employed. In these cases the prognosis must be more guarded.
Some Other Types of Meningitis
Several unusual types of meningitis may pose a significant problem in differential diagnosis. Although the meninges are rarely implicated in a hypersensitivity reaction, such involvement can occur in serum sickness and in sensitivity to certain sulfonamide drugs. A possible sensitivity to the rat lung worm, Angiostrongylus cantonensis, has beer the suggested cause of eosinophilic meningitis.
Aseptic meningitis may result from the rupture of an. intracranial epidermoid cyst or may follow the instillation of chemicals, e.g., iophendylate (Pantopaque) into the spinal subarachnoid space. Meningitis may complicate spinal anesthesia, and, rarely, a progressive adhesive arachnoiditis ensues. Pain, pareses, and impaired sensation from involvements of the spinal cord and roots are common; rarely, the arachnoiditis extends intracranially, producing cranial. nerve damage and hydrocephalus. The cause of adhesive arachnoiditis following spinal anesthesia is unknown, but contamination of the anesthetic agent with phenol or a detergent has been suggested.