Hysteria is a disturbance of behavior in which symptoms and signs of physical ill health are imitated more or less unconsciously for some personal advantage. As the phrase “more or less unconsciously” implies, hysteria may be hard to distinguish from “malingering,” in which the imitation of illness is a well-appreciated fraud. Frank malingering is rare, though, because the power of human self-deception is usually adequate to persuade a person of the validity of his own symptoms.
The only ones who can be called malingerers with any confidence are some self-mutilating patients and the remarkable pathologic liars, picturesquely called examples of the Munchausen syndrome, who travel from hospital to hospital gaining admission by means of dramatic acts of illness.Hysterical symptoms are to be seen as responses to distressing experiences. They can occur in almost any person facing danger or difficulty, especially if, as with soldiers in battle or jailed prisoners, the distress is intense and prolonged and physical symptoms can provide a viable escape. Dull-witted or immature persons with inadequate powers of introspection and self-control may produce transparently hysterical symptoms in response to milder distress, such as school difficulties or family problems.
Some of the exaggerations and elaborations of medical symptoms common in hospitalized, sick patients may be similarly interpreted as responses to the distress of illness by persons whose capacity for self-control has been weakened by somatic .illness. Hysterical symptoms can be the first manifestations of a dementing illness or of a disorders must be considered when a previously well balanced adult develops a suspiciously hysterical symptom.
Commonly, though, hysteria is a disturbance in the behavior of a person predisposed by an attention-seeking, emotionally unstable, and egocentric personality. In fact, these characteristics form what has became known as the “hysterical personality” even though hysteria can occur in other types of people, and these characteristics do not invariably produce hysterical symptoms. Most easily recognized in these people is their flair for the dramatic. They show this tendency in flamboyant dress and in exaggerated, even melodramatic, responses to questions about their symptoms.
They are never so happy as when they are the center of attention. They often work in occupations such as modeling or acting that put them in the public eye. Although hysterical personality seems more frequent in women, it is found in men, and Dr. MacDonald Critchley points to Oscar Wilde as an example. The zeal of these patients for exaggeration and drama renders them liable to hysterical behavior in response to what, seem trivial difficulties or even when simply unable to attract attention to themselves in other ways.
Hysteria Symptoms and Signs.
Many of the phenomena of somatic illness can be imitated by hysteria. The accuracy of the imitation depends on the medical sophistication of the patient. A doctor or nurse is more likely to produce a convincing imitation than is an unqualified person.Common hysterical symptoms are vague subjective disorders, such as generalized weakness, dizziness, indigestion, or pain. Hysterical pain can occur in any part of the body, but the head and neck, the region over the heart, and the low back are particularly favored.
Hysterical pain can be of any character, from dull aching to sharp and stabbing pain, but it is often described by the patient in vivid similes such as “like a bullet,” “like a bolt of lightning,” “aches like an abscessed tooth,” or “sore as a hot boil.” Usually, hysterical pain is not confined to a local area as around a pathologic lesion, nor is it referred into the distribution of a particular nerve or dermatome.
Rather, hysterical pain is felt in a general region, of the body and spreads, sometimes in bizarre ways, into contiguous areas without regard to neuroanatomic boundaries. Thus, pain beginning in the face may spread along the side of the head and into the back, crossing from the region of the trigeminal nerve into the upper cervical nerve regions. Hysterical pain often varies in its character, intensity, and distribution, changing considerably with attention or suggestion.
Occasionally it can be remarkably improved by a small amount of intravenous amobarbital sodium when analgesics do not help. Characteristically, the tests of sensation often reveal that the cutaneous sensibility in a region of hysterical pain is heightened. The patient claims that light touches or pin pricks are not changed in character but are felt more acutely or sharply as though more pressu had been exerted by the examiner. This is hyperesthesia, and it is likely to be hysterical. It should be differentiated from hyperpathia, the senso . change thresholds are raised so that light stimuli are not perceived, but stimuli exceeding th threshold produce a disagreeable and prolong pain.
Although vague symptoms of a subjective kind such as pain or dizziness are the present vogue in hysteria, crude and gross symptoms are still seen.
These may be psychological, such as the amnesia or fugue states, in which, in the setting of some trouble that the patient would like to avoid or forget, his memory is partially lost. Amnesias are particularly common in soldiers in wartime. Ganser’s syndrome is an hysterical twilight state and pseudodementia, first described in prisoners by a Dresden prison doctor. It consists of a mild disturbance of consciousness and an associated behavior that seems intended to represent madness. Particularly characteristic of the Ganser syndrome are replies to questions indicating that a correct answer is known but a wrong answer chosen. On being asked how many legs a cat has. the patient answers three or five, never four.
Motor disturbances in the form of abnormal movement, disturbed gaits, seizures, or paralyses are occasionally hysterical symptoms. Hysterical seizures can usually be distinguished from epileptic ones. The patients generally do not hurt themselves, bite their tongues, or lose their urine. They do not have the typical tonic and then clonic phases of a seizure, but tend to show a dramatic flailing of the limbs. Consciousness is usually retained, and seizures hardly ever occur when the patient is alone. The EEG is normal.
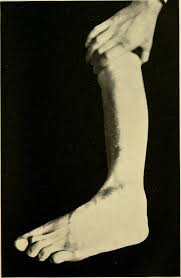
Sensory disturbances are particularly favored hysterical symptoms. Thus, blindness or deafness is common, often developing dramatically and conveniently to spare the patient embarrassment or other discomfort. Loss of sensation over one side of the body to pin prick or light touch is frequently found after a susceptible patient has been examined by a neurologist.
How TO Diagnosed Hysteria
Diagnosis of hysteria is seldom easy and never popular. Ideally, it should rest or. three supports: first, the form of the hysterical manifestation; second, the personality of the patient; and third, the setting in which the symptoms developed. Often it is not possible to find all three supports to a diagnosis, but all should be sought.
Commonly, hysterical symptoms are vague and variable. In fact, the more definite and consistent a patient’s description of the onset, location, nature, and duration of his symptoms, the less likely the symptoms are to be hysterical. Hysterical symptoms and signs are also usually incompatible with what is known of anatomy and physiology.
Thus, sensory losses do not conform to patterns of nerve distribution; reflexes remain intact and unchanged in the palsies of arm and leg; seizures of the entire body do not disturb consciousness; total blindness appears without a disturbance of pupillary reflex or of optokinetic nystagmus. The hysterically mute person can phonate on coughing. The hysterically deaf person speaks louder to be heard over increased ambient noises. Many other hysterical symptoms have been analyzed for such inconsistencies by Head.
Knowledge of the personality and past history of the patient is helpful to a diagnosis of hysteria. The recognition that the symptoms are occurring in an hysterical personality should prompt an observer to look very closely at the symptoms before embarking on extensive laboratory tests or upon surgery. Similarly, knowledge of a previous vague and poorly understood medical disturbance can lend weight to an opinion that a new symptom that has eluded diagnosis is occurring in an individual prone to hysteria. Conversely, hysteria can usually be eliminated as an explanation for symptoms in a responsible, stable, middle-aged person. People who have passed through adolescence and young adulthood without resorting to hysterical behavior are unlikely to employ it when older.
The setting in which the symptoms develop should be carefully scrutinized, and a search made for a distressing event that may have provoked an hysterical reaction or for any purpose that the hysterical symptoms may serve. Occasionally, a clear association between the symptoms chosen and a particular recent disturbance in the life of the subject can be found, such as an amnesia developing in a person who has done something shameful or criminal, or weakness and pain persisting in a person who is seeking financial compensation f r an injury.
Often, though, motivations behind hysterical symptoms are vague and uncertain. They may depend only upon a generally unhappy life situation in a person who employs hysterical symptoms to call attention and bring sympathy to himself and his present state. Also, it may be possible to demonstrate that the development of particular symptoms has been prompted by suggestion: weakness of legs, for example, developing in a nurse caring for a paraplegic patient, or peculiar falling attacks after the patient has witnessed an epileptic seizure.
A careful study of the symptoms, the personality, and the life setting of a patient usually allows a reasonably certain differentiation of hysterical symptoms from those of a medical illness. There are, however, certain medical problems that are notoriously easily confused with hysteria. These are the diseases that produce vague and changing symptoms that seem to vary with the patient’s motivation and, at least in their early phases, lack convincing physical signs.
If such an illness occurs in a patient who has features of the hysterical personality and who will therefore describe the symptoms in a dramatic and flamboyant fashion, physicians may be even more persuaded to believe that the illness is only deceptively physical.
Examples of diseases frequently confused with hysteria because of their subtle clinical features are the first attack of multiple sclerosis, particularly if sensory changes alone are produced; the weakness of arms and legs seen early in acute idiopathic polyneuritis of the Guillain-Barre type; the difficulty in swallowing of bulbar myasthenia gravis; the attacks of muscular weakness in periodic paralysis; the tonic posturings and oculogyric crises of postencephalitic parkinsonism; the pain of a cauda equina tumor; and the abdominal pain-of acute intermittent porphyria.
Management of Hysteria.
The management of hysterical patients is difficult. No one method can be recommended unqualifiedly. But there are certain principles that can be followed. To help hysterical patients it is essential to have sympathy for them. Many doctors find these patients irritating. It is just as possible to see them as individuals displaying an intriguing aspect qt human behavior that could be almost comical if it did not have such tragic implications in their live’S. It is pointless to argue with these patients about the validity of their symptoms. A useful approach is to agree that they have had an illness producing their symptoms, but that they are now improving even though total recovery has not arrived.
It is important to diagnose hysteria promptly.
Hesitation in diagnosis leading to several hospital admissions for extensive laboratory investigations is a good way to solidify hysterical symptoms in a patient. Among other things, the uncertainty of doctors helps persuade a patient that the symptoms are real. Repeated examinations increase the consistency with which symptoms are reported. Long hospitalization, mounting bills, and the inconvenience caused to others make it difficult for a patient to abandon symptoms without embarrassment. The gratifyi: g attention given to the patient in the hospital, perhaps as an example of an intriguing diagnostic problem, can feed the self- dramatizing tendencies and so encourage the behavior.
There is always risk in any diagnosis since diagnosis is only a weighing of probabilities. The diagnosis of hysteria, though, depends purely on a physician’s judgment and, before relief of symptoms is accomplished, can be confirmed in the laboratory only by evidence of health. Physicians, for obvious reasons, fear more the error of calling a physically sick patient hysterical than the error of mishandling hysteria.
They often- prefer to exclude, by laboratory examination, progressively more unlikely diseases than to study carefully the symptoms and the individual who has produced them, even though this would lead more directly to a definite diagnosis as well as an understanding of the response. It may be unwise to counsel too strongly against this behavior because medical diagnosis is never easy. A compromise can be found in the admonition to perform immediately the laboratory tests that seem necessary for a patient, but when hysteria is suspected, to bring the period of investigation as quickly as possible to a close so that management of the specific symptom can be begun.