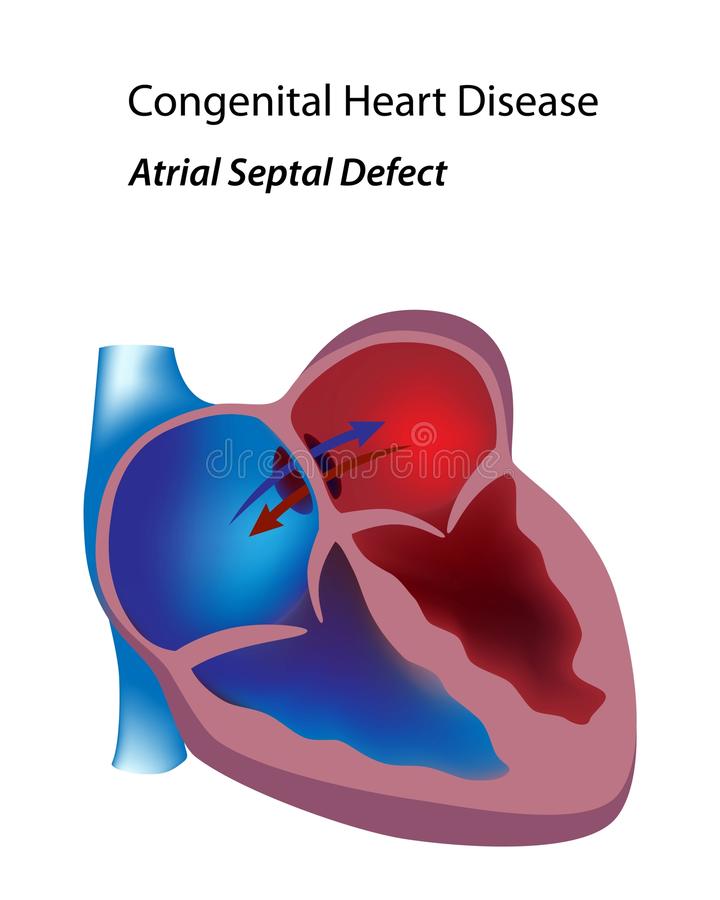
Atrial septal defect occur more frequently in females and are designated according to their site in the septum. The most common are in the region of the fossa ovalis (ostium secundum defect) and are among the most prevalent congenital cardiac anomalies in adults. A less frequent variety (sinus ivnosus defect) occupies the upper part of the atrial septum and is closely related to the entry of the superior vena cava. This structure receives one or more anomalously draining pulmonary veins, usually from the right lung.

The principal factors that determine the magnitude of the left to nght shunt are the size of the defect, the relative compliance of the cardiac chambers, and the vascular resistances in the pulmonary and systemic circulations. If the defect is moderate or large 2 cm in diameter in an adult), the greater distensibility of the right atrium and ventricle and the low pulmonary vascular resistance allow a torrential left to right shunt. On the other hand, in infancy the relatively thick and less compliant right ventricle limits the magnitude of left to right shunts. Large defects with torrential left to right shunts produce right atnal and ventricular enlargement, which encroaches on the left-sided chambers. Pulmonary pressures and resistances are generally normal. In the unusual instances in which they are elevated, the pulmonary circulation remains vasoactive, so that pressures and resistances return to normal after surgical ablation of the shunt. Those with severe pulmonary vascular disease are described under Eisenmenger Syndrome.
Diagnosis of Atrial Septal Defect
Although symptoms are trivial and physical signs subtle, the diagnosis is usually made during childhood. However, many escape detection in the first decade of life and are recognized in later years only because of effort dyspnea and fatigue. Superimposed coronary artery disease or systemic hypertension can cause the left ventricle to be less distensible, favoring the development or worsening of these symptoms because of a further increase in left to nght shunt and right volume overload.
In some instances the presence of the defect is first appreciated when pulmonary hypertension develops with persistence of a torrential left to right shunt. The advent of atnal arrhythmias, fibrillation, flutter, or paroxysms of supraventricular tachycardia is not well tolerated. These events increase in frequency beyond the fourth decade. Some patients with an uncomplicated atrial septal defect are recognized for the first time because of an abnormal “routine” chest roentgenogram.
In children failure to gain weight is common but by no means the rule. The characteristic physical appearance is that of a thin child with nearly normal height and a gracile habitus. Generally adults have a normal physical appearance but again some arethin and gracile. The jugular venous pulse shows “a” and “v” waves of equal heights because the atria are in free communication. Dominant “a” waves suggest the presence of pulmonary hypertension, and dominant “v” waves are associated with tricuspid regurgitation. Right ventncular volume overload results in an easily palpable left parasternal lift.
The importance of this sign cannot be overemphasized and in some the dilated pulmonary artery is palpated in the second left interspace. The soft ejection systolic murmur, seldom accompanied by a thrill, is best heard at the upper left sternal edge and is produced by increased blood flow into the pulmonary artery The murmur, especially a loud one, is widely transmitted to the chest anteriorly and posteriorly, especially in slightly built patients. The murmur is preceded by an accentuated first heart sound and sometimes by a pulmonic ejection sound. The auscultatory hallmark is the easily audible, widely split second heart sound. This split is virtually fixed in all phases of respiration and dunng the Valsalva maneuver. When the defect is large, a middiastolic murmur is audible at the lower left sternal edge and is produced by torrential flow across the tricuspid valve. An early diastolic murmur of pulmonary regurgitation may accompany pulmonary hypertension, but this is rare.
The electrocardiogram shows right axis deviation and right ventricular hypertrophy (generally rsR’ in right precordial leads). This pattern is due to terminal depolarization of the hypertrophied right ventricular outflow tract. Less frequent findings include tall P waves (because of right atrial enlargement), complete right bundle branch block, a prolonged P-R interval, and Wolff-Parkinson-White syndrome. Supraventricular arrhythmias may be detected in untreated adults or many years after surgical closure of the defect. These consist of atrial fibrillation or flutter, paroxysmal atrial tachycardia, and multiple premature atnal contractions. Left axis deviation usually denotes the presence of an ostium primum atrial defect but is seen occasionally in secundum defects. Another rare finding is a normal electrocardiogram.
Treatment of Atrial Septal Defect
Treatment is surgical ablation of the shunt, especially when the pulmonary systemic flow ratio exceeds 2:1 This is preferably accomplished between the ages ol about 3 and 4 years, when the surgical risk 15 minimal In these young patients the nght ventncular dimension returns to normal Surgical treatment in older children and adolescents usually improves the size of the night sided chambers. but they may not return to normal When the operation is performed in adults, patchy fibrosis of the chronically volume-loaded right ventricle persists, as does some degree ol nght ventncular dilatation.
These residua may explain the blunted chronotropic response during exercise. with resultant decreased cardiac output and decreased working capacity. Nevertheless patients in the filth, sixth. o» even seventh decade with high pulmonary blood flow and low resistance benefit from surgical repair, which can be done with a comparatively low.