
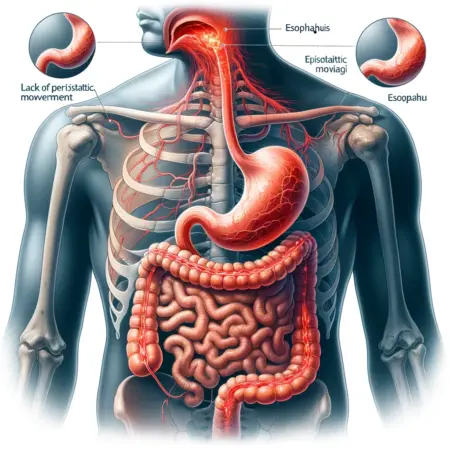
Apcristalsis is a chronic disorder of motility which leads to obstruction at the level of the esophagogastric. It is actually inappropriate, as the “cardiac” sphincter (or vestibule) is not contracted with excessive force, but only fails to relax (achalasia) in the act of swallowing. Moreover, it is clear that the disturbance of motility also involves the lower two-thirds of the body of the esophagus, where the normal progressive wave of contraction fails to develop on swallowing. Thus the most inclusive and satisfactory concept, including the absence both of moving waves of contraction and of receptive relaxation, is that of aperistalsia of the esophagus.
Prevalence of Aperistalsis.
Although one of the more common causes of esophageal obstruction, apcristalsis is a relatively rare disease in medical practice in the United States, where no regional, ethnic or familial predisposition has been recognized. It develops usually in the third to sixth decades, and is rare in children. No environmental factors of otiologic importance are known.
In Latin America, however, an identical disorder occurs endemically among the poor, chiefly in rural districts, in whom an association with Chagas’ disease is suggested by epidemiologic and serologic evidence. In such patients the esophageal disorder is often associated with disturtiances elsewhere, such as megaureter or megacolon and
Pathological And Physiology of Aperistalsis
The fundamental lesion in a|x*i istalsis. whether idiopathic or related to Chagas’ disease, is degeneration of the ganglion cells of the myenteric (Auerbach’s) plexus of the esophagus. This varies greatly in degree, at times amounting to complete atrophy and at times being undetectable by ordinary histologic criteria, and appears to Ik* proportional to the duration and seventy of the motility disturbance.
With failure of relaxation of the vestibule on swallowing, food and liquid accumulate in the esophagus until, in the vertical position, the hydrostatic pressure exceeds the resistam-e of the sphincter, and the contents passes bit by bit into the stomach. The esophagus may I to greatly dilated and elongated but. if the level of total motor activity is high, may long remain of normal caliber. The wall of the esophagus often becomes greatly thickened, although just above the vestibule conspicuous thinning or a pseudodiverticulum may appear. With severe retention, the mucosa and submucosa an* often inflamed. Rarely, carcinoma of the lower esophagus appears to In* a complication of longstanding megaesophagus. Because patients often lie down before the esophagus empties itself. acute and chronic aspiration pneumonia is a moderatelv common comolieation.
Clinical Manifestations of Aperistalsis
The leading symptom. dysphagia, is usually insidious in onset; but in many instances it may begin suddenly and may intermittent or of variable severity, despite the persistence of the morphologic anti physiologic changes in the esophagus. Exacerbations are often correlated with xriods of life stress and emotional tension; even the need to eat a meal hastily or away from homo may heighten the distress. The dysphagia is likely to progress in severity, but not steadily as in organic strictures. From the Beginning, some difficulty will Ik* experienced in swallowing liquids as well as solids. Nevertheless, the patient often learns that he can obtain relief by drinking a liquid after a meal, presumably because the added fluid raises the hydrostatic pressure in the lower esophagus sufficiently to open the sphincter. Substemal after eating, lasting a few minutes, occurs variably in some patients, apparently because of spasm of the body of the esophagus.
Diagnosis of Aperistalsis
The symptom of dysphagia should lead promptly to tho performance of a Ixirium swallow; in a typical case of advanced aperistalsis the dilated, elongated, tortuous body of the esophagus, together with an elongated, 1 irmly contracted vestibule, permits easy recognition. Sometimes the disease is suspected because the esophagus produces the shadow of a large paramediastinal mass on plain film of the chest. When the esophagus is less strikingly enlarged, fluoroscopic study in tin* horizontal |K>sition will still reveal defects in the primary peristaltic wave, and “spot” films of the terminal esophagus will show the point of narrowing as a symmetrically tapered cone. Ksopha-goscopy confirms this and, l>eoause the vestibule usually dilates to allow passage of the instrument into the stomach, permits exclusion of an organic stricture.
Manometric studies of swallowing may be of great diagnostic value, showing the typical disturbances in motility of the sphincter and the body of the esophagus, as well as spasmodic contraction of the body on subcutaneous injection of methacholine. In some cases with minimal dilatation of the esophagus, it is impossible to make a clear distinction between aperistalsis and diffuse esophageal spasm on the clinical and manometric findings.
By those moans, aperistalsis can and must be differentiated from carcinoma of the fundus of the stomach or terminal esophagus. In such instances. during endoscopy direct biopsy of tho lesion or (IxMter) cytologic study of aspirated contents may reveal neoplastic cells. In scleroderma of tho esophagus comparable defects in peristalsis are seen in the body of tho esophagus, but the vestibular sphincter is most often patent and there is no abnormal sensitivity to metharholine. In regurgitant esophagitis the manometric findings are not typical of aperistalsis, and evidence of regurgitation, of mucosal inflammation, of stricture, or of hiatal hernia is usually obtained by fluoroscopic study, by esophagoscopy and by measuring the pH of the lower esophageal contents.
Treatment and Prognosis of Aperistalsis
Initial conservative management is recommended because many patients are able to eat adequately and with minimal distress when freed from stress and emotional tension. Such cases should lx* treated patiently and sympathetically by the methods of simple psychotherapy (see article on Irritable Colon). The only medication frequently useful is a mild sedative. Anticholinergic drugs, such as atropine sulfate 0.5 to 1.0 mg., or propantheline 15 to .10 mg., can prevent or relieve painful spasms of the body of the esophagus. but do not relax the esophagogastric sphincter. Amyl nitrite inhalation (or glyceryl trinitrite. 0.4 mg. sublingually) relaxes the sphincter: nevertheless, because this effect is variable and transient and peristalsis is not restored. it is of little practical importance.
The damage done to the innervation of the esophagus in this disease is. nevertheless, irreversible. and truly effective therapy requires that this compensated by lasting damage to the esophagogastric sphincter, permitting drainage of the esophagus by gravity. Forcible stretching or rupture of the muscle fibers is accomplished bv bougies and other dilators passed and positioned in the sphincter under fluoroscopic control. The most effective of these is the Starck dilator, which is forced open like an umbrella.
The procedure is painful, but in experienced hands the risk of perforation of the esophagus is small, and the vast majority of patients obtain lasting relief. Pneumatic bags may also Ik* employed successfully. These procedures are recommended for any case of aperistalsis in which severe* dilatation and significant retention are regularly present and in which accurate placement of the dilator is technically feasible.
When adequate dilatation has not been possible or its results have lxH*n unsatisfactory, surgical division of the sphincter often lieeomes necessary. Vet the more radical and successful tho destruction of the sphincter, the more likely is the postoperative occurrence of regurgitant esophagitis (discussed later), hero worsen<*d by the ineffective clearing of regurgitated material causc of defective peristalsis.