Angina pectoris is a clinical syndrome caused by inadequate oxygenation of the heart, characteristically precipitated by exertion, and relieved by rest or sublingual nitroglycerin. Although there were several earlier reports, the condition since known as angina pectoris was masterfully described by William Heberden in 1772 in a paper entitled “Some Account of a Disorder of the Breast.” The word angina refers to the sensation of strangling and anxiety which accompanies an attack.
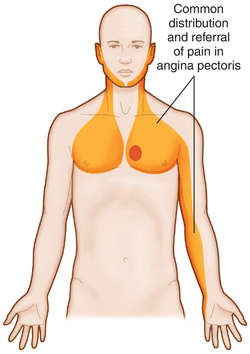
Heberden pointed out that the condition is common; that the seizure occurs while walking, especially uphill or after a meal; that the uneasiness vanishes with standing still; that prior to an attack the subjects appear perfectly well; that the pain is in the sternal area but may go to the left arm; that males past 50 are the most common victims; and that sudden death may terminate an attack.
Angina Pectoris Clinical Manifestations.
Pain. The discomfort of angina may vary from mild to most intense. It may per- sist as a vague ache, and although the patient is aware of the sensation, he may continue his activities. On the other hand, once started, angina may rapidly build up to the point of intolerance, forcing the victim to stop and seek immediate relief. The pain of angina is usually not as severe as the intense precordial crushing sensation associated with acute myocardial infarction. It is usually described as pressing, boring, or gripping. The patient may feel as though a weight is on his chest.
Precipitating Factors.
Angina is characteristically episodic and triggered by physical activity. A patient may be able to predict discomfort by a specific act, for ex- ample, climbing a flight of stairs, but in other patients the effort of exertion is variable. Walking may be tolerated, but climbing a small hill may precipitate an at- tack. Angina is frequently induced by a heavy meal, especially if followed by exertion. Some patients are forced to change their habits and eat several small meals to avoid discomfort. Cold weather is especially prone to produce angina. Sometimes the first contact with cold air on leaving a warm room is sufficient, even though the patient is standing still. Many patients are able to walk indoors and perform labor, although they cannot do the same outdoors without discomfort.
Causes of Angina Pectoris
Many theories have been proposed in an attempt to explain the mechanism of cardiac pain. It is most likely directly related to metabolic changes caused by ischemia. Electrocardiographic abnormalities may precede awareness of’ pain or may occur in absence of’ pain, suggesting that an accumulation of active sub- stances to some threshold necessary to cause pain is occurring. Such substances might be W, , and possible components of the kallikrein system. There are two networks of sensory nerve fibers in the heart: a perivaseular network encircling the coronary arteries, and fibers running beside the vessels and terminating be- tween muscle bundles. Presumably the latter are stimulated by the ischemic process.
The pain of angina pectoris and that of myocardial infarction are similar in quality. The pain of infarction tends to be more intense, and may persist for several hours. Prolonged pain implies continued ischemia, not infarction. Once death of myocardium has occurred, pain is no longer present. One explanation for the occasional sudden improvement in previously stable angina is infarction of the chronically ischemic area. Ischemic cardiac pain and the pain of intermittent claudication presumably have a similar mechanism. Both are described as deep, visceral sensations. Both occur with increased muscular work and are relieved by rest. Both are usually secondary to obstructive vascular disease.
Pathogenesis.
According to current understanding, angina pectoris develops when cardiac work, and hence myocardial oxygen need, is greater than the ability of the coronary arterial system to supply oxygen per unit time, Angina can be precipitated by an increase in cardiac work and hence oxygen need, or, conversely, angina may occur after a decrease in the oxygen supply secondary to obstruction of coronary flow or a reduction of arterial oxygen content. It most commonly results when cardiac work and hence myocardial oxygen need exceed the available oxygen supply because coronary blood flow to certain regions is restricted. Obstruction of coronary flow owing to coronary atherosclerosis is the most common anatomic finding in the presence of angina. Other conditions which greatly increase cardiac work, such as aortic stenosis, hypertrophic subaortic stenosis, and aortic regurgitation, may be associated with angina despite anatomically normal coronary arteries.
Diagnosis of Angina Pectoris
Angina pectoris is a clinical diagnosis, largely dependent on the history. In some cases the diagnosis may be established by direct observations during an attack. In the vast majority of patients, however, the diagnosis is evident to the experienced physician from the history alone, and confirmatory tests are not needed. The electrocardiogram may be utilized to confirm the diagnosis. In doubtful cases the recording of typical electrocardiographic “ischemic” changes, as described earlier, during an attack of pain will often be diagnostic. However, use of exercise tolerance tests with electrocardiographic recording to confirm the presence or absence of angina is frequently unsatisfactory. Occurrence of pain, the patient’s actual complaint, is uncommon. As discussed earlier, it is important that the test be standardized and closely monitored. A positive test, in the absence of pain, does not confirm the presence of angina. It does suggest, however, the presence of ischemic or coronary artery disease.
The response to nitroglycerin may be utilized as a critical diagnostic test. Angina pectoris is characteristically relieved in from 90 seconds to 3 minutes after sublingual administration of nitroglycerin. Failure of the symptom to be relieved promptly by nitroglycerin should cast suspicion on the diagnosis of angina. Many patients have a poor sense of timing, and cannot accurately describe the duration of an attack or the quickness of relief after medication. It is important to emphasize to the patient the necessity for accurate information before drawing the GT’nclusion that nitroglycerin is not useful and therefore that the diagnosis is in doubt.
Angina Pectoris Treatment.
An effective plan of treatment must be based on a thorough understanding of the severity and intensity of the patient’s complaint. The physician should explore carefully the circumstances in which angina occurs. Often, minor adjustments in the patient’s activity will reduce the frequency of attacks. Angina often occurs repeatedly during the same activity. Avoidance of that specific activity or administration of nitroglycerin before onset will usually reduce symptoms. Should an attack occur, most patients will stop, rest, and administer a nitroglycerin tablet. Some will ignore the discomfort and continue their exertion.
Progressive increase in intensity of pain usually forces the subject to stop. Occasionally the pain will improve despite continued activity. Although the development of angina usually indicates significant obstruction of one or more vessels by coronary atherosclerosis, it is important to emphasize the generally good prognosis in patients with stable angina. The patient should be encouraged to report any change in the pattern of angina promptly to his physician.
Angina pectoris is a medical condition characterized by chest pain due to reduced blood flow to the heart. Here’s a tabular format outlining its causes, diagnosis, and treatment:
| Aspect | Details |
|---|---|
| Causes | – Coronary artery disease (narrowing of the coronary arteries) |
| – Atherosclerosis (buildup of plaque in arteries) | |
| – Spasm of coronary arteries | |
| – Anemia | |
| – Extreme physical exertion or stress | |
| Diagnosis | – Medical history and physical examination |
| – Electrocardiogram (ECG) | |
| – Stress testing (exercise stress tests) | |
| – Echocardiogram | |
| – Blood tests (to check for markers of heart damage) | |
| – Coronary angiography (for detailed artery imaging) | |
| Treatment | – Lifestyle changes (diet, exercise, smoking cessation) |
| – Medications (nitrates, beta-blockers, calcium channel blockers, antiplatelet drugs, statins) | |
| – Percutaneous coronary intervention (PCI) or angioplasty (to open narrowed arteries) | |
| – Coronary artery bypass grafting (CABG) for severe cases | |
| – Management of underlying conditions (like hypertension, high cholesterol, diabetes) |
This table provides a structured overview of angina pectoris, including its common causes, diagnostic methods, and various treatment options.